1. Introduction
According to estimates from the International
Telecommunication Union, the number of worldwide mobile cellular
subscriptions increased from 68.0 per 100 inhabitants in 2009 to
108.0 per 100 inhabitants in 2019 [
1]. With the increasing use of
cellular phones, concerns have arisen over the carcinogenic
effects of electromagnetic fields (EMFs) emitted from cellular
phones [
2]. Since 1999, observational
epidemiologic studies, specifically case-control studies have
reported inconsistent findings on the association between
cellular phone use and tumor risk, and several meta-analyses [
3,
4,
5,
6] of case-control studies on
this topic have been published before 2011.
Among these studies, Myung et al.’s
meta-analysis [
5] of 23 case-control studies
concluded that mobile phone use was associated with an increased
tumor risk in high quality studies and studies conducted by a
specific research group, and that long-term mobile phone use of
10 or more years increased the risk of tumors regardless of
methodological quality or research group. Similarly, Khurana et
al. also reported that cellular phone use of 10 or more years
doubled the risk of brain tumors in 11 epidemiologic studies [
6].
Based on evaluation of the available
literature including experimental animal studies and
epidemiological studies in humans, in 2011, the World Health
Organization (WHO)/International Agency for Research on Cancer
(IARC) classified radiofrequency electromagnetic fields
(RF-EMFs) associated with cellular phone use as possibly
carcinogenic to humans [
7]. Recently, an advisory group
of 29 scientists recommended that IARC prioritize a new review
of the carcinogenicity of RF-EMF by 2024 due to mechanistic
evidence of the carcinogenicity of cell phone radiation
published since 2011 [
8].
Although many case-control studies and several
meta-analyses have been published regarding the association
between cellular phone use and tumor risk, the findings remain
inconsistent.
The purpose of this study was to evaluate the
associations between cellular phone use and tumor risk using a
systematic review and meta-analysis of case-control studies
according to various factors including differences in response
rates between cases and controls, use of blinding at interview
for ascertainment of exposure, methodological quality, funding
sources, type of case-control study, malignancy of tumor, and
dose–response relationship.
3. Results
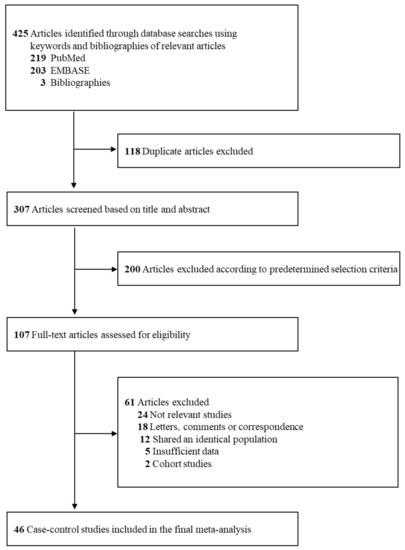
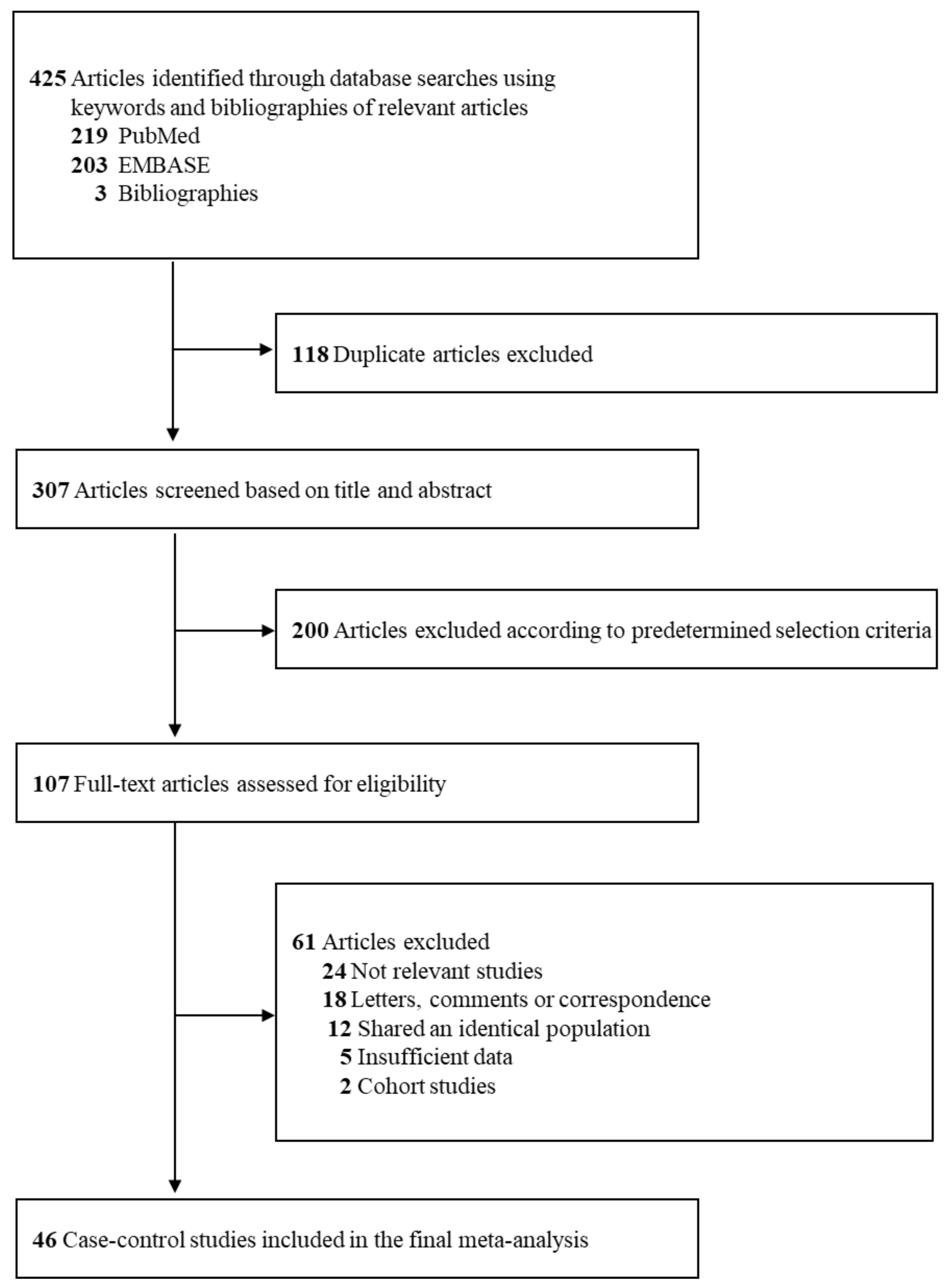
3.1. Study Selection
shows a flow
diagram for the selection process of relevant studies. We
identified a total of 425 articles from three core databases
with 219 articles from PubMed, 203 articles from EMBASE, and 3
articles from hand-search. After excluding 118 duplicate
articles and 200 articles that did not satisfy the
pre-determined selection criteria by reviewing those titles
and abstracts, the full texts of the remaining 107 articles
were assessed for the final selection. After reviewing the
full texts, 61 articles were excluded for the following
reasons: not relevant studies (n
= 24), letters, comments, or correspondence (n
= 18), shared an identical population (n
= 12), insufficient data (n =
5), and cohort studies (n =
2). The remaining 46 case-control studies (13–58) were
included in the final analysis.
Figure 1.
Study selection.
3.2. General Characteristics of Studies and Participants
General characteristics of the case-control
studies included in the meta-analysis are shown in . The 46
case-control studies involved a total of 66,075 participants
with 24,717 cases and 41,358 controls. For studies reporting
gender, 53.9% of study participants were women. A total of 37
studies were hospital-based case-control studies, while nine
studies were population-based case-control studies. The
included studies were conducted in the following countries:
Sweden (n = 24), Denmark (n = 9), United Kingdom (n
= 8), Finland (n = 7), Norway
(n = 6), Germany (n
= 5), US (n = 4), Israel (n = 3), Japan (n
= 2), Italy (n = 2), New
Zealand (n = 2), France (n = 2), Brazil (n
= 1), China (n = 1), South
Korea (n = 1), and Thailand (n = 1). The most common type of
tumor in the included studies was brain tumor (34 out of 46
studies, 74%), and the next most common ones were head and
neck cancer such as parotid gland tumor (5/46, 12%),
hematologic malignancies such as leukemia and non-Hodgkin’s
lymphoma (4/46, 8.7%), melanoma (2/46, 4.3%), and testicular
cancer (1/46, 2.2%).
Table 1.
General characteristics of studies included in the
meta-analysis (n = 46).
The studies were classified by research
group, i.e., Hardell studies (
n
= 11), INTERPHONE studies (
n
= 19), and studies conducted by other groups (
n
= 16). As shown in
Table S1 and
Table S2, the NOS scores ranged between
4 and 8 (average score, 6.4), and the NHLBI quality assessment
scores ranged between 6 and 10 (average score, 8.3). We
considered studies with an NOS score of ≥7 stars or an NHLBI
quality assessment score of ≥9 points as having high quality
and the remaining studies as having low quality.
The Hardell studies were not funded by the
cellular phone industry. Most had high scores of ≥7 stars in
the NOS and high scores of ≥9 points in the NHLBI quality
assessment; most reported high response rates (>70%) with
smaller differences in response rates (<14.5%) between the
case group and the control group; and all were
population-based case-control studies (,
Table S1, and
Table S2). All of the INTERPHONE
studies were partly funded by the cellular phone industry
(precisely, supported by funding from the International Union
against Cancer, which received funds from the Mobile
Manufacturers’ Forum and Global System for Mobile
Communications Association) except for the INTERPHONE-Japan
studies. Most had low scores of <7 stars and low scores of
<9 points, showed low response rates (<70%), and had
larger differences in response rates (>14.5%) between the
case group and the control group. All were population-based
case-control studies (,
Table S1, and
Table S2).
Table 2.
Use of cellular phones and risk of tumors in subgroup
meta-analysis of case-control studies.
No study conducted by the other groups was
funded by the cellular phone industry. Most of these studies
had low response rates and mainly larger differences in
response rates between the case group and the control group ().
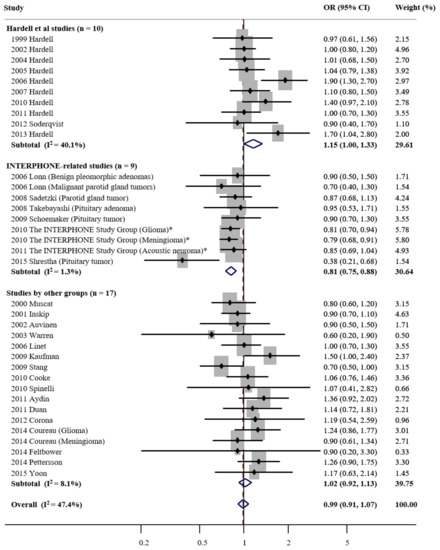
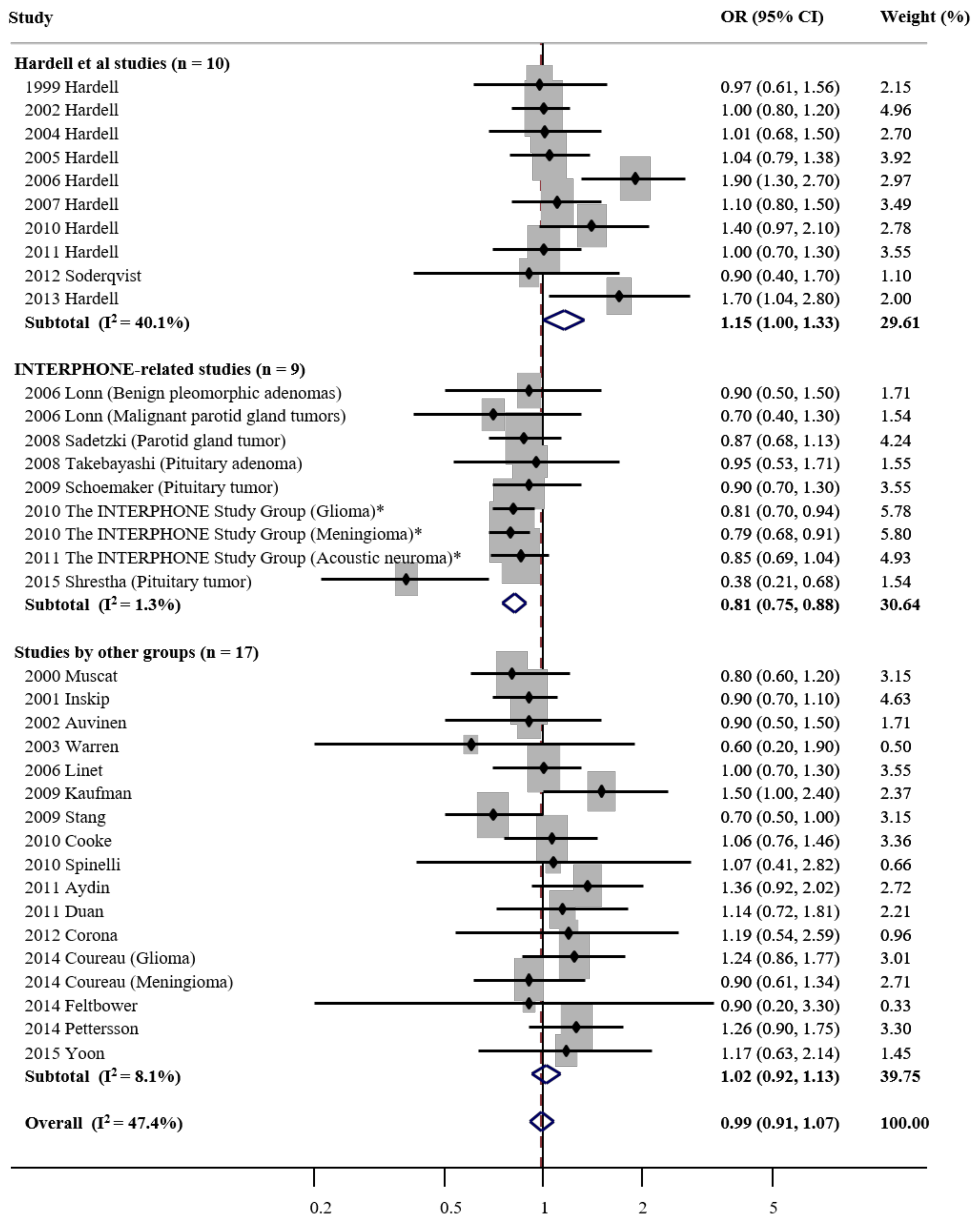
3.3. Overall Use of Cellular Phone and Risk of Tumors
As shown in , as compared
with never or none, the overall use of cellular phones was not
associated with tumor risk in a random-effects meta-analysis
of all 36 studies (OR, 0.99; 95% CI, 0.91 to 1.07; I
2
= 47.4). Of the 46 studies, several [
24,
25,
26,
27,
28,
29,
30,
32,
33,
34,
35,
36] were excluded from the
main analysis but included in the subgroup meta-analysis
because study subjects overlapped with the INTERPHONE study
published in 2010 [
40] and 2011 [
41] (which reported pooled
results from all 13 countries).
Figure 2.
Cellular phone use and risk of tumors in a random-effects
subgroup meta-analysis of case-control studies by research
groups (n = 36). OR—odds
ratio; CI—confidence interval. *—2010 and 2011 The
INTERPHONE Study Group studies involved 13 countries.
In the subgroup meta-analysis by research
group, cellular phone use was associated with marginally
increased tumor risk in the Hardell studies (OR, 1.15 (95% CI,
1.00 to 1.33; n = 10; I2
= 40.1%), whereas it was associated with decreased tumor risk
in the INTERPHONE studies (OR, 0.81; 95% CI, 0.75 to 0.88; n = 9; I2 = 1.3%). In
the studies conducted by other groups, there was no
statistically significant association between the cellular
phone use and tumor risk (OR, 1.02; 95% CI, 0.92 to 1.13; n = 17; I2 = 8.1%).
Publication bias was not observed overall
(Begg’s funnel plot was symmetric; Egger’s test, p
for bias = 0.07). In addition, there was no publication bias
in the subgroup meta-analysis by research group (Egger’s test,
p for bias = 0.36 in the
Hardell studies, 0.57 in the INTERPHONE studies, and 0.68 in
studies by other groups, respectively).
3.4. Use of Cellular Phones and Risk of Tumors in Subgroup
Meta-analysis By Various Factors
shows the
findings of the subgroup meta-analyses by various factors.
Cellular phone use was statistically significantly associated
with increased tumor risk in studies that used blinding at
interview (OR, 1.16; 95% CI, 1.01 to 1.34; n
= 10; I2 = 39.4%). In addition, cellular phone use
had a marginally statistically significant association with
increased tumor risk in studies with high methodological
quality (OR, 1.11; 95% CI, 1.00 to 1.22; n
= 17; I2 = 20.1%, based on the NOS score; OR, 1.09;
95% CI, 0.99 to 1.20; n =
20; I2 = 29.3, based on the NHLBI quality
assessment tool). In contrast, cellular phone use had
statistically significant associations with reduced tumor risk
in studies that did not use blinding at interview, or were
rated as having low methodological quality. Both the NOS score
and NHLBI quality assessment tool showed similar findings in
methodological quality scores: most Hardell studies were rated
high quality, while most INTERPHONE studies were rated low
quality.
Similarly, subgroup meta-analyses by funding
source revealed a non-significant increased risk of tumors by
cellular phone use in studies not funded by the cellular phone
industry (OR, 1.07; 95% CI, 0.98 to 1.17; n
= 28; I2 = 21.9%), whereas a statistically
significantly decreased risk of tumors was observed in studies
partly funded by the cellular phone industry (OR, 0.81; 95%
CI, 0.74 to 0.89; n = 8; I2
= 0%), all of which were INTERPHONE studies.
Cellular phone use was not statistically
significantly associated with tumor risk in the subgroup
meta-analysis by type of case-control study. In the subgroup
meta-analysis by type of tumor, a significantly decreased risk
of benign tumors was observed (OR, 0.86; 95% CI, 0.77 to 0.95;
n = 14; I2 =
21.9), while no significant association was observed for
malignant tumors. This decreased risk of benign tumors was
only found in INTERPHONE studies, not in Hardell et al.
studies and studies by other groups.
3.5. Exposure–Response Relationship Between Use of Cellular
Phones and Risk of Tumors
shows an
exposure-response relationship between cellular phone use and
tumor risk. In the subgroup meta-analysis by time since first
use or latency, overall the risk of tumors by cellular phone
use non-significantly increased from an OR of 0.97 to 1.29 as
latency increased from less than 5 years to 10 or more years.
This finding was observed in each subgroup meta-analysis by
research group. Especially, statistically significant
increased tumor risk was observed for latency of 10 or more
years in the Hardell studies (OR, 1.62; 1.03 to 2.57; n
= 5; I2 = 39.9%). Similarly, the use of cellular
phones non-significantly increased the risk of tumors as the
cumulative or lifetime use in years and the cumulative number
of calls increased in all studies and in each study group.
Remarkably, in the subgroup meta-analysis of all studies by
cumulative call time, cellular phone use greater than 1000 h
statistically significantly increased the risk of tumors (OR,
1.60; 1.12 to 2.30; n = 8; I2
= 74.5%). Interestingly, the use of cellular phones overall
and in the Hardell studies (OR, 3.65; 1.69 to 7.85; n
= 2, especially in the Hardell studies) non significantly
increased the risk of tumors with cumulative call time of
300–1000 h and more than 1000 h, while it decreased the risk
of tumors in most subgroup meta-analyses of the INTERPHONE
studies.
Table 3.
Exposure–response relationship between use of cellular
phones and risk of tumors.
3.6. Use of Cellular Phones and Risk of Tumors in Subgroup
Meta-analysis By Type of Tumor
Table S3 shows the findings from the
subgroup meta-analyses by type of tumor. There was no
statistically significant association between cellular phone
use and tumor risk in most subgroup meta-analyses. Increased
tumor risk was found for malignant brain tumors only in the
Hardell studies (OR, 1.35; 95% CI, 1.06 to 1.73;
n
= 5; I
2 = 53.9%).
4. Discussion
In this comprehensive systematic review and
meta-analysis, we found statistically significant differences in
the findings for the association between cellular phone use and
tumor risk which varied by research group. Namely, there was a
statistically significant increased association by 15% in the
Hardell studies, a statistically significant decreased
association by 19% in the INTERPHONE studies (multi-national
case-control studies coordinated by the IARC), and no
significant association in the other research groups’ studies.
Importantly, in the subgroup meta-analysis of all studies
reporting cumulative call times greater than 1000 h, cellular
phone use with cumulative call time greater than 1000 h (about
17 min per day over a 10 year period) increased the risk of
tumors by 60%.
Perhaps due to methodological deficiencies,
cellular phone use appeared to reduce tumor risk in the
INTERPHONE studies. These studies were partly funded by the
mobile industry, had poor methodological quality, showed larger
differences in response rates between the case and control
groups, and did not use blinding at interview.
A substantial research literature documents
potential mechanisms for the effects of cellular phone use on
tumor risk. Although heating is the only biological effect of
non-ionizing radiation (NIR) (including microwave radiation from
cellular phones) recognized by most health agencies, numerous in
vitro studies and animal studies demonstrated other possible
mechanisms including increasing oxidative DNA damage and
altering protein structure and expression [
59]. In addition to a human
endothelial cell line study, a human volunteer study reported a
local exposure of human skin to RF-EMF caused changes in protein
expression [
60].
Based on the findings from pre-clinical
studies, previous observational epidemiological studies, mainly
case-control studies have reported inconsistent findings on the
associations between cellular phone use and tumor risk. In 2009,
we first reported evidence linking mobile phone use to increased
tumor risk in a meta-analysis of low-biased case-control
studies, especially among mobile phone users of 10 years or
longer [
5]. Two years later, the
WHO/IARC classified RF-EMF due to cellular phone use as Group
2B, or “possibly carcinogenic to humans.” [
7] Since then, subsequent
case-control studies have reported inconsistent findings
regarding the association between cellular phone use (use vs.
never or rarely use) and tumor risk, similar to our previous
findings. Since we published our meta-analysis in 2009, six
meta-analyses [
61,
62,
63,
64,
65,
66] have reported the
associations between cellular phone use and risk of brain tumors
or head and neck tumors, mainly glioma and salivary gland
tumors. Among them, four meta-analyses concluded that there was
a statistically significant increased risk of glioma among heavy
or long-term (over 10 years) mobile phone users in meta-analyses
of 10 to 12 case-control studies [
61,
64,
65,
66]. In addition, one [
62] of the remaining
meta-analyses demonstrated a statistically significantly higher
risk of all types of intracranial tumors in long-term mobile
phone users (over 10 years) in a meta-analysis of 24
case-control studies, and the other [
63] reported a statistically
significantly increased risk of parotid gland tumors in a
meta-analysis of three case-control studies.
Although the above mentioned four recent
meta-analyses of case-control studies reported a significant
increased risk of glioma in heavy or long-term (over 10 years)
mobile phone users with an odds ratio of 1.35 in Wang et al. [
61], 1.44 in Yang et al. [
64], 1.33 in Wang et al. [
65], and 1.33 in Prasad et al.
[
66], our study found a
non-significantly increased risk with an OR of 1.66. This
difference is due to the following reasons: Wang et al.’s
meta-analysis in 2016 [
61] reported that a significant
association was found between mobile phone use of more than 5
years and glioma risk (OR = 1.35; 95% CI, 1.09 to 1.62;
p
< 0.05). However, when we reviewed the main results and in their article,
the OR with 95% CI for mobile phone use of more than 5 years was
1.64 with 1.12 to 2.15. More importantly, when we performed a
random-effects meta-analysis using the same data used in their
analysis, there was no significant association between long-term
use (>5 years) of mobile phones (the correct OR with 95% CI
was 1.12 with 0.80 to 1.56). Yang et al.’s meta-analysis in 2017
[
64] used seven studies
comprising a Hardell study, a study by another group, and five
INTERPHONE studies for long-term mobile phone use of 10 years or
longer. The five INTERPHONE studies [
26,
27,
29,
30,
34] were four publications [
26,
27,
29,
30] from individual countries
(Denmark, Sweden, UK, and Germany) and one publication [
34] of a collaborative analysis
from five countries (Denmark, Finland, Norway, Sweden, and UK)
within the same study years (2000–2004). Thus, Yang et al. used
identical populations in three countries (Denmark, Sweden, and
UK) in duplicates and used a smaller dataset from five countries
instead of collaborative data [
40] on glioma for the
INTERPHONE studies from 13 countries published in 2010. When we
performed a meta-analysis using the 2010′s collaborative data [
40] instead of the five studies
used in Yang et al.’s analysis, which were partly duplicated and
smaller in sample size and number of countries than the 2010
collaborative analysis of the INTERPHONE group, there was no
significant association between long-term mobile use and the
risk of glioma (OR, 1.49; 95% CI, 0.80 to 2.78;
n
= 3; I
2 = 91.5%), which is closer to our finding.
Wang et al.’s meta-analysis in 2018 [
65] included two cohort studies
as well as case-control studies. More importantly, they included
four ORs of >10–15 years, >15–20 years, >20–25 years,
and >25 years from Hardell’s 2015 study [
67]. If each OR is calculated
from independent data (not overlapping), they can be combined.
However, each reference used for the calculation of each OR was
overlapping. When we conducted a meta-analysis using only an OR
of 1.40 for 10–15 years of wireless phone use in Hardell’s 2015
study based on the Wang et al. analysis, there was no
significant association between long-term use and the risk of
glioma (OR, 1.08; 95% CI, 0.90 to 1.30;
n
= 6; I
2 = 49.2%).
Compared to previous meta-analyses, the
current meta-analysis has several strengths. First, the current
meta-analysis is the most comprehensive study conducted to date,
as it included 46 case-control studies with various types of
tumors other than brain tumors. Second, we performed critical
subgroup meta-analyses by factors that could affect individual
results, such as the difference in response rates between cases
and controls and funding sources, as well as use of blinding at
interview for ascertainment of exposure and methodological
quality. From these crucial subgroup meta-analyses, we confirmed
that the opposite findings between the Hardell studies
(increased tumor risk among cellular phone users) and the
INTERPHONE studies (decreased tumor risk among cellular phone
users) were closely associated with these factors. The
INTERPHONE studies had differential response rates in case and
control groups, did not use blinding at interview, had low
methodological quality scores, and were partly funded by the
cellular phone industry. In contrast, the Hardell studies had
comparable response rates in case and control groups, used
blinding at interview, had high methodological quality, and had
no industry funding. Although there was no statistical
significance, similar findings were observed in the subgroup
meta-analysis by the above mentioned factors in the studies by
other groups. In the current main analysis of 36 case-control
studies, nine out of 10 Hardell studies showed smaller
differences in response rates between case and control groups
and had high response rates of about 80–90% in both groups. In
contrast, all of the INTERPHONE studies showed larger
differences in response rates between both groups; most had
lower response rates in the control group than in the case
group, and most had low response rates of about 40–70%. Over the
past decades, participation rates (response rates in this study)
have decreased in case-control studies, particularly in
controls, which could lead to non-representative selection of
controls, reducing the validity of the effect estimates, and
casting doubt on the veracity of study findings [
68]. Thus, the decreased risks
of tumors observed in the INTERPHONE studies might be due to
selection bias from participation of cellular phone users in the
control group [
69]. We also found that studies
partly funded by the cellular phone industry showed a
statistically significantly decreased risk of tumors by cellular
phone use, all of which were INTERPHONE studies. It remains
unclear whether cellular phone industry funding affected the
study planning and conduct or data analysis and interpretation
because the authors reported that the provision of funds to the
study investigators via the UICC was governed by agreements that
guaranteed INTERPHONE’s complete scientific independence.
Nonetheless, many of these investigators rely upon industry for
future research funding so they may have “hidden conflicts” of
interest despite such agreements [
70].
Our meta-analysis is based upon case-control
studies which potentially suffer from recall bias and selection
bias. Although prospective cohort studies typically enable
stronger inferences to be drawn regarding causality, these
studies are difficult to conduct when the outcome is a rare
chronic disease that requires long-term exposure and subjects
are exposed to multiple potential toxins. So far, two
prospective cohort studies have been published [
71,
72]. Both employed inadequate
measures of cell phone use, and one misclassified many cell
phone users as non-users [
71]. A large, international
prospective cohort study is ongoing but will not yield results
on tumor risk for 20 or more years [
73].
There are several limitations in the current
study. Although cordless phones often have a much higher power
output than cellular phones, and the users of analogue phones
have used longer than those of digital phones, we excluded the
impact of those phones in this analysis. This might lead to a
bias that underestimates the effect of mobile phones on the risk
of cancer. In addition, we did not consider ipsilateral and
contralateral use of the cellular phones, which is beyond the
scope of our study. Lastly, although we reported
exposure-response relationships between the cellular phone use
and the cancer risk, it would be ideal to investigate those
associations based on the actual time spent on cellular phones
provided by the mobile telecommunication companies. However,
most studies did not use those data. Further studies using the
exact data on the time spent on cellular phones are warranted to
confirm our findings.





{kind=link}
{kind=link}